


Key Takeaways
- Accuracy is Mandatory: Your notes are legal documents that prove the care you provided.
- Structure Matters: Using formats like SOAP helps keep your documentation organized and clear.
- AI Can Help: Tools like Norma act as a coach to improve your phrasing and vocabulary.
- Objectivity is Key: Focus on what you see, hear, and measure rather than personal opinions.
- Consistency: Regular, detailed entries protect both the resident and your professional license.
Documentation is a fundamental part of your role as a healthcare professional. It serves as the primary communication tool between care teams and provides a permanent record of resident care. When you write clear nursing progress notes, you protect your residents, your facility, and yourself.
However, finding the right words during a busy shift is difficult. You might struggle to describe a complex behavior or explain an incident without sounding subjective. This is where modern tools come in. By pairing traditional documentation standards with advanced technology, you can improve the quality of your notes significantly.
The Critical Role of Clinical Documentation
Your notes do more than just fill space in a file. They tell the story of the resident's health journey. When you document effectively, you support the entire care team.
Accurate records provide several benefits:
- Continuity of Care: The next shift knows exactly what happened and what needs attention.
- Legal Protection: If an incident occurs, your notes are the first thing auditors or lawyers review.
- Funding Justification: Detailed notes support claims for funding by proving the level of care delivered.
- Clinical Decision Making: Doctors and specialists rely on your observations to adjust treatments.

If you do not document an action, legally, it did not happen. This makes the quality of your writing essential.
Understanding the Legal Standards for Documentation
Legal documentation requires adherence to strict guidelines. You must write as if your notes will be read in a courtroom years from now. Vague statements or emotional language can weaken your credibility.
Follow these rules to maintain legal soundness:
- Be Objective: Only write what you observe. Avoid words like "stubborn" or "lazy." Instead, describe the behavior: "Resident refused to open mouth for medication."
- Be Timely: Write notes as soon as possible after the event. Late entries can look suspicious during an audit.
- Be Specific: Avoid general terms like "good day." Use specific measurements and descriptions.
- Use Standard Abbreviations: Only use abbreviations approved by your facility to prevent confusion.
- Sign and Date: Every entry must be attributable to you with a clear time and date stamp.
The SOAP Method: A Foundation for Success
One of the best ways to organize your thoughts is the SOAP method. This structure keeps your notes focused and logical.
Subjective (S)
This section includes what the resident or family tells you. It is their verbal report of the situation.
- Direct quotes from the resident.
- Complaints of pain or discomfort.
- Statements about feelings or preferences.
Objective (O)
This section lists factual data that you collect through observation and measurement.
- Vital signs (blood pressure, temperature, pulse).
- Physical exam findings (bruising, swelling, skin color).
- Lab results.
- Observed behaviors (crying, pacing, sleeping).
Assessment (A)
This is your clinical interpretation of the subjective and objective data. It is not a diagnosis but a summary of the problem.
- Changes in condition.
- Response to interventions.
- Status of existing problems (improved, worsening, stable).
Plan (P)
This outlines what you will do next.
- Follow-up actions.
- Referrals to other professionals.
- Changes to the care plan.
- When the next assessment will occur.
How to Use Norma to Refine Your Phrasing
Artificial intelligence has changed how we approach administrative tasks. Specifically, AI for aged care provides support that was previously unavailable to nurses on the floor. Norma is an AI assistant designed to help you find the "gold standard" phrasing for your notes.
Norma does not write the note for you from scratch without input. Instead, she acts as a mentor. She helps you translate rough thoughts into professional, legally sound language.
Step 1: Identify the Incident
Start with the raw facts of what occurred.
- Example: "Mrs. Jones fell in the bathroom. She says she's fine. No bumps on her head. I put her back to bed."
Step 2: Ask Norma for Improvements
Open the Norma chat interface. You can ask her to help you professionalize your language.
- Prompt: "Norma, I need to write a progress note for a resident fall. The resident states she is uninjured. Physical assessment shows no injury. She was assisted back to bed. How should I phrase this to meet legal standards?"
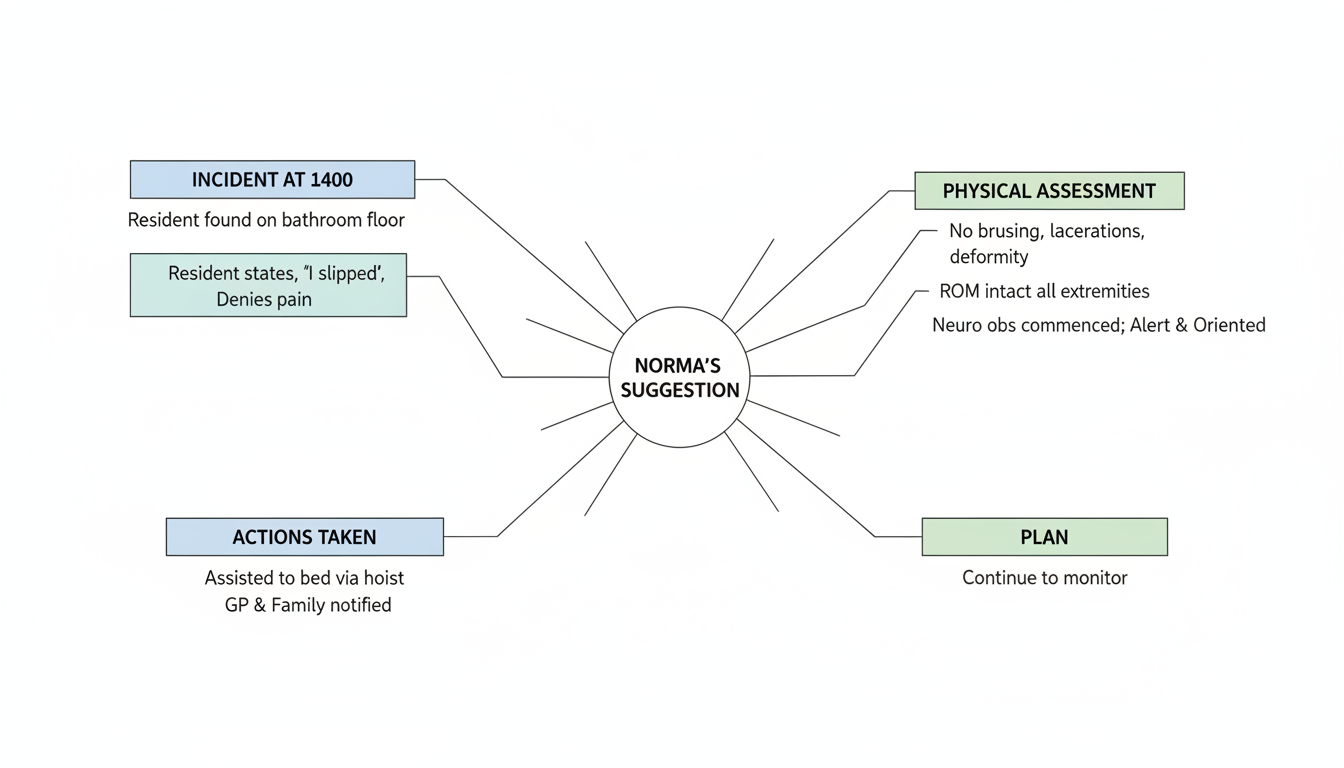
Step 3: Review the Suggestions
Norma will provide phrasing that aligns with the Strengthened Aged Care Quality Standards.
- Norma's Suggestion: "Resident found seated on bathroom floor at 1400 hours. Resident states, 'I slipped,' and denies pain or discomfort. Physical assessment conducted: no bruising, lacerations, or deformity observed. ROM intact in all extremities. Neuro observations commenced; resident alert and oriented. Assisted to bed via hoist. GP and family notified. Will continue to monitor."
Step 4: Verify Against Policy
Check the suggestion against your facility's specific policies. Norma helps you learn the correct terminology so you can use it independently in the future.
Practical Charting Examples: Good vs. Bad
Seeing examples helps clarify the difference between a poor note and a professional one. Here are charting examples to guide you.
Example 1: Refusal of Care
Poor Note: "Mr. Smith was grumpy and wouldn't take his shower. He yelled at me."
Why it fails:
- "Grumpy" is subjective.
- "Yelled at me" is vague.
- It does not explain the outcome or safety measures.
Better Note (Gold Standard): "During scheduled hygiene care, resident refused shower assistance. Resident raised voice and stated, 'Get out, I don't want to wash.' Education provided regarding skin integrity risks. Resident continued to decline. Resident left safe in room. Behavior chart updated. Will re-approach in one hour."
Example 2: Pain Management
Poor Note: "gave resident pain killer. she feels better now."
Why it fails:
- No specific medication name or dose.
- "Feels better" is not a measurable outcome.
- Grammar and capitalization errors.
Better Note (Gold Standard): "Resident complained of hip pain rated 7/10. Panadol 1g administered orally at 0900 hours. Re-evaluated at 1000 hours; resident reports pain is now 2/10 and is resting comfortably in bed. No side effects observed."
Step-by-Step: Writing a Note with AI Assistance
You can integrate AI into your daily workflow to save time while maintaining high standards. Follow this routine to write SOAP notes effectively using Norma.
- Gather Your Data: Before you sit down, make sure you have the vitals, quotes, and observation times ready.
- Open Norma: Access the bot on your device.
- Input Context: Tell Norma the situation. For example, "I need to document a wound dressing change where the wound looks smaller but has more exudate."
- Request Terminology: Ask, "What clinical terms describe a wound with yellow discharge?" Norma might suggest terms like "purulent" or "serous."
- Draft the Note: Write your note using the professional terms Norma suggested.
- Final Polish: Paste your draft into Norma and ask, "Does this note sound objective and professional?" She will highlight any emotional or vague words you missed.
Common Mistakes to Avoid in Medical Records
Even experienced nurses make mistakes. Being aware of these pitfalls helps you avoid them.
Subjective Language
Avoid using words that describe character rather than behavior.
- Avoid: Aggressive, sweet, demanding, annoying.
- Use: Struck out, cooperative, requests frequent assistance, pressed call bell 10 times in one hour.
Copy and Paste
Never copy and paste a note from a previous day or another resident. This is a major red flag for auditors. It suggests you did not assess the resident on the current shift.
Leaving Gaps
Do not leave blank lines in handwritten notes. Someone else could fill them in later. If typing electronically, make sure you complete all required fields.
Blaming Others
Medical records are not the place to complain about staffing or colleagues.
- Avoid: "Medication late because night shift didn't restock trolley."
- Use: "Medication administered at 0930 due to unavailability of stock at 0800."
Ignoring the Care Plan
Your notes must reflect the care plan. If the plan says "Assist of 2," and you document "Assisted of 1," you create a liability issue.
Frequently Asked Questions
What should I do if I make a mistake in a handwritten note?
Draw a single line through the error so it is still readable. Write "error" above it and initial it. Never use white-out or scribble over the text completely.
How often should I write progress notes?
This depends on your facility's policy and the resident's acuity. Generally, you should write a note whenever there is a change in condition, an incident, a medical visit, or a refusal of care.
Can Norma write the note for me?
Norma can suggest phrasing and structure, but you must verify the accuracy. You are responsible for the content of the note. The AI is a tool to support your professional judgment, not replace it.
Is it okay to use abbreviations?
Only use the abbreviations that are on your facility's approved list. Using unauthorized abbreviations can lead to dangerous misinterpretations by other staff members.
What is the most important part of a progress note?
The most important part is the objective data. This includes what you saw, what you did, and how the resident responded. This factual evidence supports your clinical decisions.
Final Thoughts on Modern Documentation
Writing high-quality documentation is a skill that takes time to master. It requires a shift in mindset from simple reporting to professional, legal accountability. By focusing on objective facts and using structured formats like SOAP, you improve the safety and quality of care for your residents.
Technology is here to assist you in this process. Tools like Norma allow you to check your work against gold standards instantly. This gives you confidence that your notes are legally sound and clinically precise. When you master the art of the progress note, you become a stronger advocate for your residents and a more effective leader on your floor.
